What is Trauma-Informed Care?
Trauma-informed care understands and considers the pervasive nature of trauma and promotes environments of healing and recovery rather than practices and services that may inadvertently re-traumatize.
Graphic by the UB School of Social Work's Institute on Trauma and Trauma-Informed Care (2024)
Trauma-Informed Care
Trauma-informed care (TIC) is an organizational change process that requires all individuals, practices and protocols, and environments to engage in universal precaution for trauma. Similar to how healthcare professionals put on gloves when needing to touch patients as universal precautions for pathogens, being trauma-informed requires putting on metaphorical gloves by changing interactions, policies and environments to prevent the possibility of re-traumatization.1
Organizations that use a trauma-informed approach fully integrate awareness of individual, historical, racial and systemic trauma into all aspects of functioning to provide environments for everyone in the organization that intentionally reduce the likelihood of further harm and allow opportunity for healing and growth. All layers of the organization demonstrate a paradigm shift from asking, “What is wrong with you?” to “What has happened to you?” 2-3

Graphic by the UB School of Social Work's Institute on Trauma and Trauma-Informed Care (2022)
Being trauma-informed requires an active, ongoing commitment on behalf of all members of the organization to maintaining a basic understanding of trauma and adversity, recognizing and reflecting on how one’s self-view and worldview influence their interpretation of the here and now, acknowledging that being trauma-informed is about the workforce as much as it is about individuals receiving services, and a commitment to a planful, organizational strategy for the work.
Re-traumatization
Re-traumatization refers to any procedure, interaction, situation or environment that replicates someone’s history of trauma literally or symbolically — activating the body’s survival (fight, flight or freeze) response, and activating the emotion, body responses and cognitions associated with the original experience(s).1,4 Due to the high prevalence of adversity and trauma, the potential for re-traumatization exists within all systems, and at all levels of systems: for individuals, staff and at the organization or system level.
Re-traumatization is usually unintentional. There are some more “obvious” practices that may be re-traumatizing, such as the use of restraints or isolation. However, less obvious practices or situations that involve specific smells, sounds or interactions that replicate themes (such as being unseen/unheard, non-acknowledgement of work-related stress, non-transparency) can also result in re-traumatization.3
Additionally, individuals who are part of groups that have experienced historical, racial, systemic and/or intergenerational trauma can experience re-traumatization from exclusionary practices, practices without cultural and/or accessibility considerations, microaggressions, non-inclusive language, etc.1

Chart by the UB School of Social Work's Institute on Trauma and Trauma-Informed Care (2021)
We have learned that the way we do business often hurts people.4 Re-traumatization not only causes additional harm, but is also associated with less engagement in services, higher rates of self-harm and injury in individuals receiving services, staff turnover, lower staff morale and reduced organizational commitment.4-6
Universal Precaution: Values and Principles of Trauma-Informed Care
Applying the values and principles of trauma-informed care allows for individuals and organizations to reduce the likelihood of re-traumatization.3 Neutralizing the potential of re-traumatization in interactions, policies, procedures and environments not only helps to prevent doing further harm, but also allows the possibility for resilience, healing and growth.1
The five guiding trauma-informed values and principles proposed by Drs. Maxine Harris and Roger Fallot are safety (physical and emotional), trustworthiness, choice, collaboration and empowerment.
Given the presence of individual, historical, racial, cultural and systemic trauma, true universal precaution requires that considerations of diversity, equity, inclusion, accessibility and justice (DEIAJ) are centered when applying the values and principles in our work.
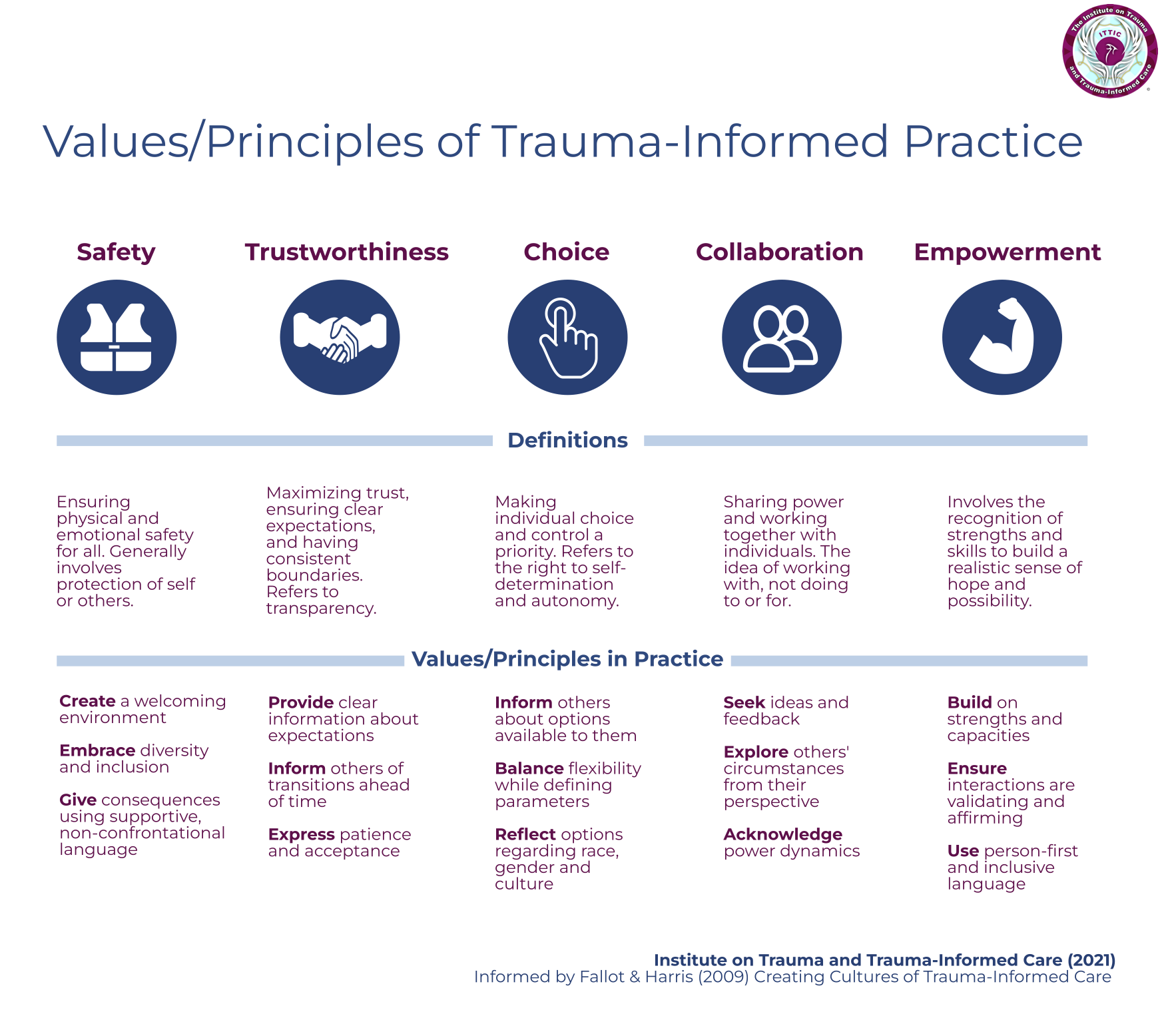
Chart by the UB School of Social Work's Institute on Trauma and Trauma-Informed Care (2021)
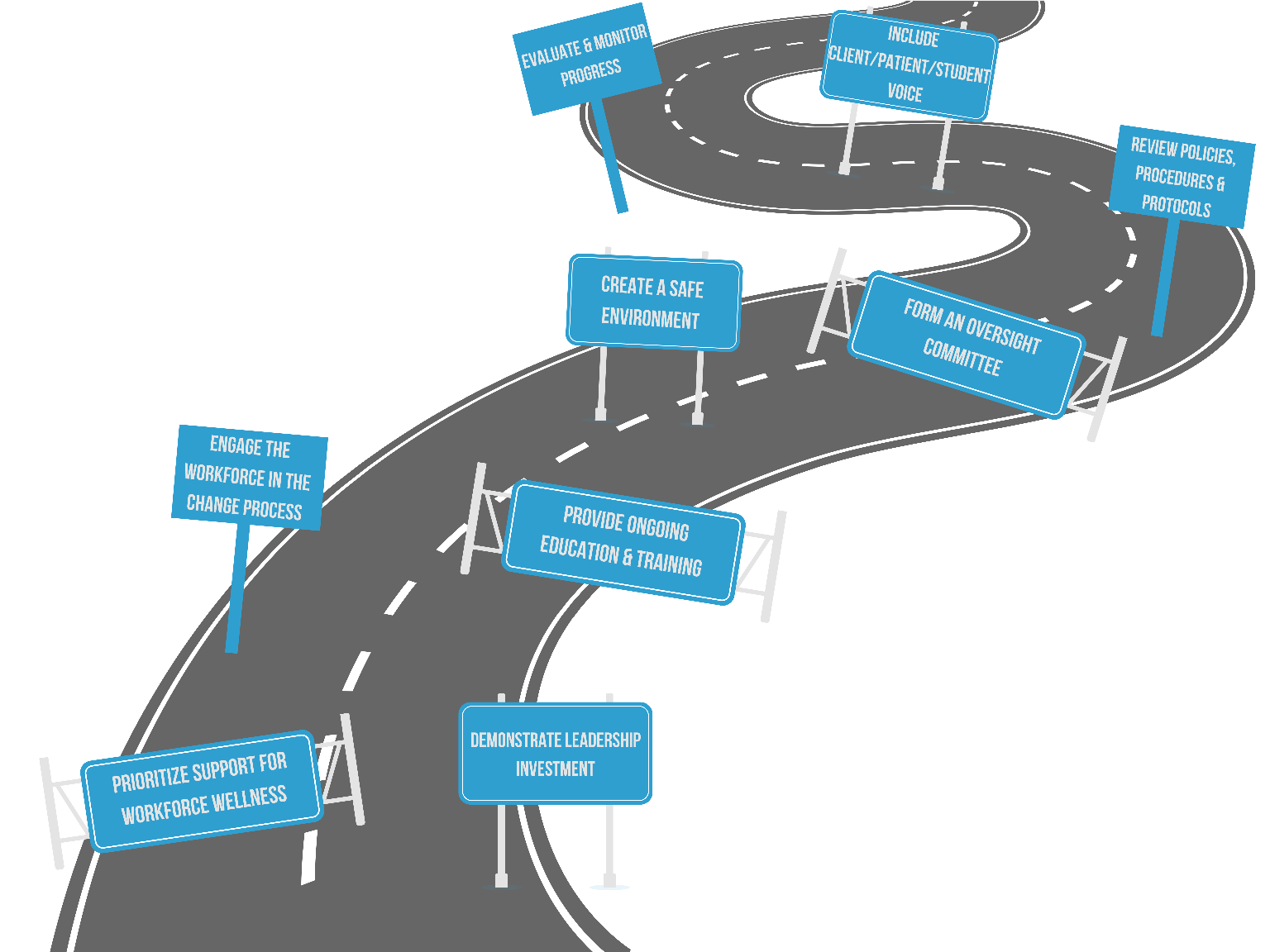
Key Components of a Trauma-Informed Organization
Organizations looking to become more trauma-informed need to apply the filter of the trauma-informed values and principles with integrated DEIAJ considerations to all levels of the organization.1-3,6-7 This requires an intentional and ongoing review of the various aspects of organizational functioning, such as the physical environment, policies and procedures, communication and messaging mechanisms, considerations for screening and treatment of trauma, and evaluation of the change process.
While becoming a trauma-informed organization is best equated to a journey rather than a destination, it typically takes a minimum of three to five years for organizations to embed trauma-informed values and principles into all aspects of functioning.1,7 The UB Institute on Trauma and Trauma-Informed Care’s trauma-informed organizational model provides a framework for organizations to build on what they are already doing that is in alignment with being trauma-informed and create a roadmap within 10 key development areas to deepen their implementation.
For more information and tools to implement trauma-informed organizational change within the 10 key development areas, consider requesting ITTIC’s Trauma-Informed Organizational Change Manual.
References
- Koury, S. P., Green, S. A., & Way, I. (2022). Trauma-informed organizational change manual. The Institute on Trauma and Trauma-Informed Care. https://socialwork.buffalo.edu/trauma-manual
- Bloom, S. L. (2013). Creating sanctuary: Toward the evolution of sane societies. Routledge.
- Harris, M., & Fallot, R. D. (Eds.). (2001). Using trauma theory to design service systems. New directions for mental health services. Jossey-Bass.
- Jennings, A. (2009). Models for developing trauma-informed behavioral health systems and trauma-specific services: 2008 update. National Center for Trauma-Informed Care. http://www.theannainstitute.org/Models%20for%20Developing%20Traums-Report%201-09-09%20_FINAL_.pdf
- Bloom, S. L. (2010). Organizational stress as a barrier to trauma-informed service delivery. In Becker, M. and Levin, B. (Eds.), A Public Health Perspective of Women’s Mental Health (pp. 259-311). Springer.
- Substance Abuse and Mental Health Services Administration. (2014). TIP 57: Trauma-informed care in behavioral health services. https://store.samhsa.gov/product/TIP-57-Trauma-Informed-Care-in-Behavioral-Health-Services/SMA14-4816
- Substance Abuse and Mental Health Services Administration. (2023). Practical guide for implementing a trauma-informed approach.